PROTECT | Values Guided Suicide Prevention
HEALING WITH HOPE | A Journey of Mental Wellbeing, Resilience, and Connection
Welcome to PROTECT, a transformative podcast dedicated to nurturing mental well-being, building resilience, and fostering hope. At its core, PROTECT is about the power of human connection—exploring how values like compassion, belonging, and loyalty can become lifelines for those facing challenges. Founded on the principle of Relational Safety, this podcast moves beyond traditional perspectives, asking not “what’s the matter with you?” but “what matters to you?”—empowering both professionals and individuals in their journey to chip away at pain and build strength.
Hosted by Dr. Manaan Kar Ray, an innovator and leader in mental health crisis care with over a decade of experience at Oxford and Cambridge, and now the Director of Mental Health Services at Princess Alexandra Hospital, Brisbane, PROTECT is changing the way we think about suicide prevention. Each episode blends leading-edge research with person-centered practice, bringing insights that promote hope, purpose, and resilience.
In our new focus, we introduce the STEPS 4 HOPE podcast series—an intimate exploration of suicide prevention through story, metaphor, and values-based connection. This season follows Ari’s Tapestry, a narrative journey through the six STEPS of suicidal distress: FABRIC, THREAD, NEEDLE, TIP, MEND, and FLOW. Each episode blends poetic storytelling, clinical insight, and emotional resonance to help listeners better understand what risk feels like—and how to respond with presence, curiosity, and care. Grounded in the HOPE framework, this series is a companion for anyone seeking to support others through pain, or to reweave their own path forward.
Whether you’re a clinician, caregiver, educator, or someone walking your own recovery journey, this podcast is an essential resource for all those who care deeply about mental health, suicide prevention, and building communities that thrive on connection and kindness.
Further information at www.PROGRESS.guide.
PROTECT | Values Guided Suicide Prevention
15 | AWARE 2 - Rational vs Rationalizing
Would love to hear your thoughts...
This episode introduces the listeners to a key concept, the 2 mental spaces in which an assessor operates in an assessment.
Rational - facts followed by decision
Rationalizing - decision followed by fact selection
Manaan uses a range of practical examples to elaborate decision making processes including Festinger's original research from 1954 and the fascinating story of scientology believers. Listen in :)
Connect with Assoc Prof Manaan Kar Ray on Linkedin
Follow us on www.progress.guide
Host: Good day, I am Mahi, your host. Welcome to episode 15 of PROTECT. We hope you have also heard and enjoyed the Guest shows we have recently hosted. Ashley P Evans with her genuine candid demeanor and Stand Steindl’s contrasting careful considered approach, both have been very popular and we would love to hear what you think, particularly if you have recommendations for future guests that you would like to listen to, on the show. You can email us at admin@progress.guide or direct message Manaan on Likedin with your suggestions for guests.
Expert: Actually, I have got another fantastic guest lined up, Linda Hipper, she is a colleague and the Director of Addiction Services at Metro South. She is a passionate advocate for addiction services and how suicide prevention frameworks do not pay enough attention to substance use and all the brief interventions that can be done in this space, interventions that are effective and enhance safety. So looking forward to interviewing her.
Host: Substance misuse and the attitudes professionals hold was something that came up in the AWARE study too.
Expert: Yes that’s true and we will be discussing that today, I have always felt that there is more that we need to do in terms of brief interventions for Alcohol and other drugs. In fact in the SAFE framework the A stands for access to means, alcohol and other drugs, but often the Access to Means discussion ends up taking all the limelight and the Alcohol and Other Drugs discussion gets overshadowed, so it will be good to have Linda early in the piece to share her wisdom, she did warn me to say that I might get an earful.
Host: That’s something to look forward to indeed, well in the last episode we discussed Anxiety, the first of the 5 AWARE factors, we finished the last show on an important note - Do you see what you want to see, or do you dare to open yourself up to all that is there to see.
Expert: I think the context was anxiety and what is it that makes professionals seek out safety reassurances and ask can you keep yourself safe, They all know that risk is dynamic and when someone says yes I can, really that yes is only valid till the circumstances remain the same and as soon as the person in distress leaves the consulting room the circumstances change, but the practice carries on, and it carries on because the desire to quell anxiety is a powerful psychological force.
Host: And that is the point you were making regarding how once a safety reassurance is received, the intent to keep digging and unearthing challenges in the near future dissipates, cause although knowledge of those challenges are essential for safety planning, they would inherently give rise to anxiety again.
Expert: That is correct, unnamed or unidentified or unaddressed anxiety in a professional may result in superficial assessments, cause the more you know the more anxious you may feel. There is another way to quell that anxiety, quell it properly and that involves a thorough assessment, finding out all the pitfalls on the road ahead and addressing them properly. That too will decrease a professional’s anxiety. But it may be challenging in time and resource poor environments so it is easier to not dig too deep or plaster over using a safety reassurance.
Host: I get the impression that you are about to delve into rational vs rationalising, one of the key insights from the AWARE study, but before you do that may I please remind our listeners that as usual the show notes, the key messages and the messages in images are available at the podcast blog at www.progress.guide or you can get the PROTECT Guidebook from Amazon to read along. The images are particularly helpful for visual learners and help with retention. Also do not forget to rate us on spotify or apple podcast, it helps us get the word out. Ok so lets get into the meat of this episode, rational vs rationalising.
Expert: I always get excited talking about this key insight from the AWARE study, I love it because people get it, its simple and the idea of Cognitive Dissonance has been around since the 1950s. At a very simple level it can be boiled down to “We see what we want to see.” This is a theme which will recur through the entire AWARE framework. As we have been saying anxiety is not a nice emotion to experience, so there is an unconscious driver to decrease anxiety not just for the person in distress but also for the assessor themselves, we just mentioned one of the ways which is through seeking reassurances related to safety. So the shallow blanket statement ‘I can keep myself safe’ helps rationalize away why not to explore fully the dynamic aspect of risk. This is where the whole rational vs rationalizing exploration of the qualitative data started.
Host: Can you elaborate on those two terms rational and rationalizing?
Expert: Sure, as explained earlier, people presenting very similarly could end up with diametrically opposite outcomes post assessment depending on the level of residual anxiety, just the information sited is different. For example when admitting someone an assessor will often highlight the anxiety provoking predisposing, precipitating and perpetuating factors, when sending someone home for community management they will highlight the protective factors. This selective abstraction of information is the foundation of the rational vs rationalising construct.
Host: So I am assuming the examples you sited is the rationalizing part of the assessment or assessor behaviour or approach to an interaction, what is the rational part.
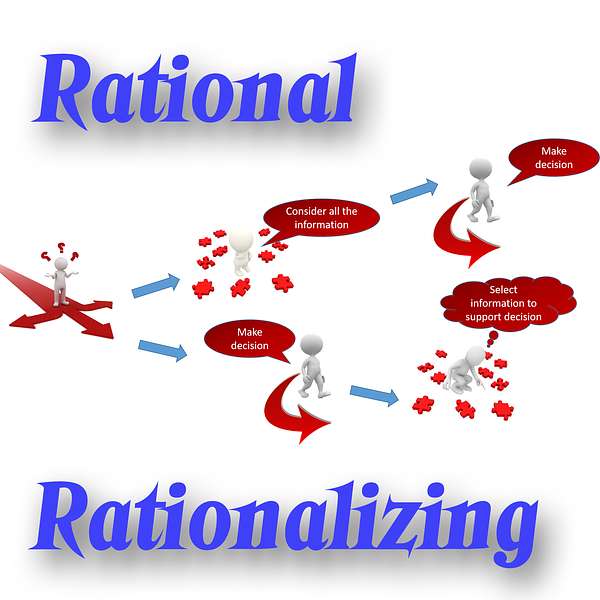
Expert: In the interviews we conducted we found two mental spaces in which the professional would operate, rational and rationalizing. In the rational space, an assessor will consider all the information they have collated, weigh up all the pros and cons and then make a decision or take action. In the rationalising space, the assessor makes a decision early on and then selectively picks out facts that are in keeping with the decision they have made.
Host: So rational is information first, decision later and rationalizing is decision first followed by selection of information to support the decision or action.
Expert: Spot on. Based on availability, assessments involve a combination of referral information, past notes, collateral information and face to face interaction. Facts in mental health are often subjective as the most important symptoms relate to the inner experiences of an individual. The collated information gets synthesised into a formulation which informs the decision how best to respond to patient needs and outstanding risks (Cooper & Oates, 2012). However, often before formulation, a hypothesis about appropriate response begins to emerge in the assessor’s mind and at a certain point crystallizes as fact. From then on, all clinical activity gets unconsciously skewed to confirm the desired outcome.
Host: Are you saying the assessment interaction actually changes because of a decision or a preliminary idea about next steps in the mind of an assessor.
Expert: Yes that’s exactly what I am implying. If you have decided early on in the assessment process what is the best outcome, it does influence which questions you will ask and even if there is a standardized questionnaire that does not stop us from interpreting the answers in the way in which we do. Even documentation skews unconsciously, to accommodate for this.
Host: So it goes back to the two mental spaces in which clinicians operate, a rational space in which fact finding is followed by decision and a rationalising space where a decision is followed by supportive facts selection.
Expert: Yes, the latter is problematic from a care allocation perspective as it creates blind spots particularly in relation to dynamic risk factors and risk factor interactions. Unfortunately, assessors are often unaware as to whether they are operating in the rational or rationalizing space (Kar Ray et al., 2018). This is a theme that plays through all the AWARE factors.
Host: Rationalising is not that dissimilar to statements like I know I am trying to lose weight but I have had a hard day’s work so I deserve that slice of sticky toffee pudding, I am guessing, action that I have rationalized through some convoluted logic, but there is that part of me that knows, “who am I kidding”.
Expert: That’s a really good example of every day rationalizing, whether it be chocolates, or that glass of wine, or the gym can wait for a day that I am not so tired, actually the gym is waiting a while till I binge watch Season 4 of Vikings. All of this is in line with Leon Festinger’s (1962) work into cognitive dissonance.
Host: You used this term before too, What is cognitive dissonance?
Expert: Most of the time we know what is the right thing to do let’s say go right, but often the right thing to do is quite hard and I want to do the opposite lets say go left. So I know I should go right but I really want to do is go left, this creates an internal struggle, not a nice place to be with a tug of war inside you. In order to eliminate the tug of war what we do is we give ourselves reasons why going left is the right thing to do, essentially giving ourselves permission to go left when in our heart of hearts we know we could have and perhaps even should have gone right.
Host: Essentially you are saying it’s the white lies we tell ourselves to convince us to take action that we know is unwise.
Expert: Or engage in inaction when we know we should doing something.
Host: It’s a bit like someone who is absolutely broke because they cannot contain their spending impulses, they know its an issue and they are working on it, they are living from pay check to pay check, they get their salary, they know that they have mouths to feed at home, they go past a jewelry shop where a beautiful necklace is at a discounted rate, they give in to their impulse, knowing full well that they will face a lot of hardships even to put food on the table and they tell themselves well this was such a bargain, look at how much money I have saved.
Expert: Yes and rationalization processes can become quite complex and convoluted, to deal with their guilt, because in their heart of hearts they know exactly what has happened, they have a spending problem and they gave into it, so they might construct an entire narrative around how this was an investment into their daughter’s future, in five years she will turn 16 and this will be her 16th birthday gift, how much joy it will bring to her at that point. Yes 2 weeks of hardship but her smiles will be priceless.
Host: This sounds like telling porky pies to ourselves.
Expert: Kind of, resolving cognitive dissonance may involve the creation of such narratives, but often these processes are unconscious. Another way of saying this is that we see what we want to see. Like someone with Bipolar disorder who always relapses when they come of their lithium, they go to a mental health library and manage to find a book written as part of the anti psychiatry movement in the 70s as to why they should not take medication and how Lithium is poisoning them, so in a library full of 100s of books that will tell them to take their medication they manage to find the one that fits in with their view of what they want to do. They have already decided what they want to do and then they keep looking till they find the information that they are looking for. Again the rationalizing processes that we saw during assessments were not so overt, the rationalizing was quite subtle but it was quite clear.
Host: I know I am deviating from the principal purpose of the podcast but this to me sounds like how conspiracy theorists must operate.
Expert: Well that is not far from the truth, if you look at Festinger’s early work there are some very interesting stories.
Host: Do share.
Expert: Perhaps a bit off track but given how important these two mental spaces are we can indulge a little bit I guess.
Festinger and his colleagues were already studying the effects of prophecy disconfirmation on groups of believers, when they read a story in a local newspaper headlined "Prophecy from Planet Clarion Call to City: Flee That Flood. It'll Swamp us on Dec. 21" The prophecy came from Dorothy Martin (1900–1992), a Chicago housewife who practiced automatic writing, and it outlined a catastrophe predicted for a specific date in their near future. Seeing an opportunity to test their theories with a contemporary case study, the research team infiltrated the group of Martin's followers in order to collect data before, during and after the time the prophecy would be disconfirmed.
Host: Don’t think this study will pass the ethics committee these days?
Expert: Come on it was the 1950s. Anyway Martin claimed to be receiving messages from superior beings from a planet she referred to as Clarion. These messages included a prophecy that Lake City and large portions of the United States, Canada, Central America and Europe would be destroyed by a flood before dawn on December 21st 1954. Through the restrained recruitment activities of Charles Laughead (a college doctor in Michigan) and other acquaintances, Martin was supported in her mediumship by a small group of believers. Some of the believers took significant actions that indicated a high degree of commitment to the prophecy. Some left or lost their jobs, neglected or ended their studies, ended relationships and friendships with non-believers, gave away money and / or disposed of possessions to prepare for their departure on a flying saucer, which they believed would rescue them and others in advance of the flood.
Host: Gosh that is some commitment.
Expert: True and as anticipated by the research team, the prophesied date passed with no sign of the predicted flood, causing a dissonance between the group's commitment to the prophecy and the unfolding reality. Different members of the group reacted in different ways. Strangely, many of those with the highest levels of belief, commitment and social support became more committed to their beliefs, began to court publicity in a way they had not before, and developed various rationalisations for the absence of the flood. Some others, with less prior conviction and commitment, and / or less access to ongoing group support, were less able to sustain or increase their previous levels of belief and involvement, and several left the group.
Host: Ah so it went both ways
Expert: Yes determined by the strength of the belief. What is interesting is the sequence of events:
December 17. Ms. Keech received a phone call from person identifying themselves as "Captain Video" from outer space, telling her that a saucer is to land in her backyard to pick her up at 4 o'clock in the afternoon. (Festinger considers this call to have been made by a practical joker reacting to press coverage of Keech's group.) Some of the group initially questioned the call, before accepting it and preparing themselves to be collected by the saucer, removing all metal objects from their persons. By 5:30 pm the group appeared to have given up, and were reluctant to discuss the issue of why the saucer had not arrived. When the matter was discussed, they agreed that the event had been a practice session. Ms. Keech received another message later that day that the saucer would pick them up at 1:30 am. The group waited for the saucer until 3:30 am then gave up. Before December 20. The group shuns publicity. Interviews are given only grudgingly. Access to Keech's house is only provided to those who can convince the group that they are true believers. The group evolves a belief system – provided by the automatic writing from the planet Clarion – to explain the details of the cataclysm, the reason for its occurrence, and the manner in which the group would be saved from the disaster. December 20. The group expects a visitor from outer space to call upon them at midnight and to escort them to a waiting spacecraft. As instructed, the group goes to great lengths to remove all metallic items from their persons. As midnight approaches, zippers, bra straps, and other objects are discarded. The group waits.
12:05 am. December 21. No visitor. Someone in the group notices that another clock in the room shows 11:55. The group agrees that it is not yet midnight.
12:10 am. The second clock strikes midnight. Still no visitor. The group sits in stunned silence. The cataclysm itself is no more than seven hours away.
4:00 am. The group has been sitting in stunned silence. A few attempts at finding explanations have failed. Keech begins to cry.
4:45 am. Another message by automatic writing is sent to Keech. It states, in effect, that the God of Earth has decided to spare the planet from destruction. The cataclysm has been called off: "The little group, sitting all night long, had spread so much light that God had saved the world from destruction."
Host: That is such a powerful story, basically there is always a reason that explains a decision or an action, it is just a matter of looking hard enough.
Expert: Yes an articulate person can essentially justify anything if they wanted to.
Host: So when making clinical decisions how do assessors mitigate the risk of slipping into the rationalizing space?
Expert: Well it starts with awareness, that’s why this framework is called AWARE. For conservative decisions assessors would maximise the risk and minimise protective factors. For decisions which involved positive risk taking, risks were minimised and protective factors were maximized. When you become aware of the inner workings of your mind you can discuss these things in supervision or reflective practice. The other important safety check in the system is the discussion post assessment with a senior or an oncall consultant, remember to stick to the facts, relay the facts not your opinion to begin with, and relay all the facts. Seek the guidance from the senior with an open mind, don’t just lead them on by presenting facts that will lead to the decision. So awareness is crucial.
Host: Seems like we have run out of time.
Expert: Well you wanted to hear Festinger’s story, but I do believe it is time well spent, rational vs rationsalising is such a critical component in terms of awareness, once you get your head around this the other AWARE factors will become much easier to understand.
Host: There you go, it is time well spent, Pause and think, the decision you have made, or the action you have taken, have you made it in the mental space that can be deemed rational, facts followed by action, or are you rationalising a decision away, so actions followed by selection of facts. Watch out for it at the dinner table, that extra portion, watch out for it in the shopping market, the shoes you don’t need, watch out for it on the road when you race the lights. Watch out for it before you scream at your child who clearly deserves to be shouted at for being on their phone at the dinner table. Make this reflective part an important part of who you are as a person and the rest in terms of clinical practice will follow. Share what you find. Tweet your thoughts about the rational and the rationalising space and tag #GuideProgress. It helps get the word out about the podcast to more professionals and support progress to practice. You can email your thoughts to us at admin@progress.guide with your suggestions and comments particularly if you have questions and want us to cover certain topics in the discussion. In the next episode, we will go through the other factors in the AWARE framework and how the two mental spaces, rational and rationalising apply to them. You can access all the information at www.progress.guide. You can connect with Manaan on Linked in, or follow our linked in page by searching on linked in for progress.guide. We are also on twitter and YouTube. Our twitter handle is @GuideProgress. As usual please do follow the podcast, there will be weekly episodes every Friday and share it with your colleagues. Your ratings will help get the word out so please don’t forget to rate us on Spotify, apple podcasts or audible or whichever channel you are listening on. Helping healthcare professionals become aware of their decision making processes is an essential step in creating a workforce that is self-aware. Remember together we can make a difference. Tune in next Friday and we will explore the other factors in the AWARE framework. Thank you for joining us today and keep spreading the word.

